0
Skip to Content
Home
About
About Us
Venue Hire
Our Team
Our Trustees
Annual Reports
AGM
Projects
Latest
Events
Monthly Calendar
News
Vacancies
Media
Video
Photos
Donate
Contact Us
Open Menu
Close Menu
Home
About
About Us
Venue Hire
Our Team
Our Trustees
Annual Reports
AGM
Projects
Latest
Events
Monthly Calendar
News
Vacancies
Media
Video
Photos
Donate
Contact Us
Open Menu
Close Menu
Home
Folder:
About
Back
About Us
Venue Hire
Our Team
Our Trustees
Annual Reports
AGM
Projects
Folder:
Latest
Back
Events
Monthly Calendar
News
Vacancies
Folder:
Media
Back
Video
Photos
Donate
Contact Us
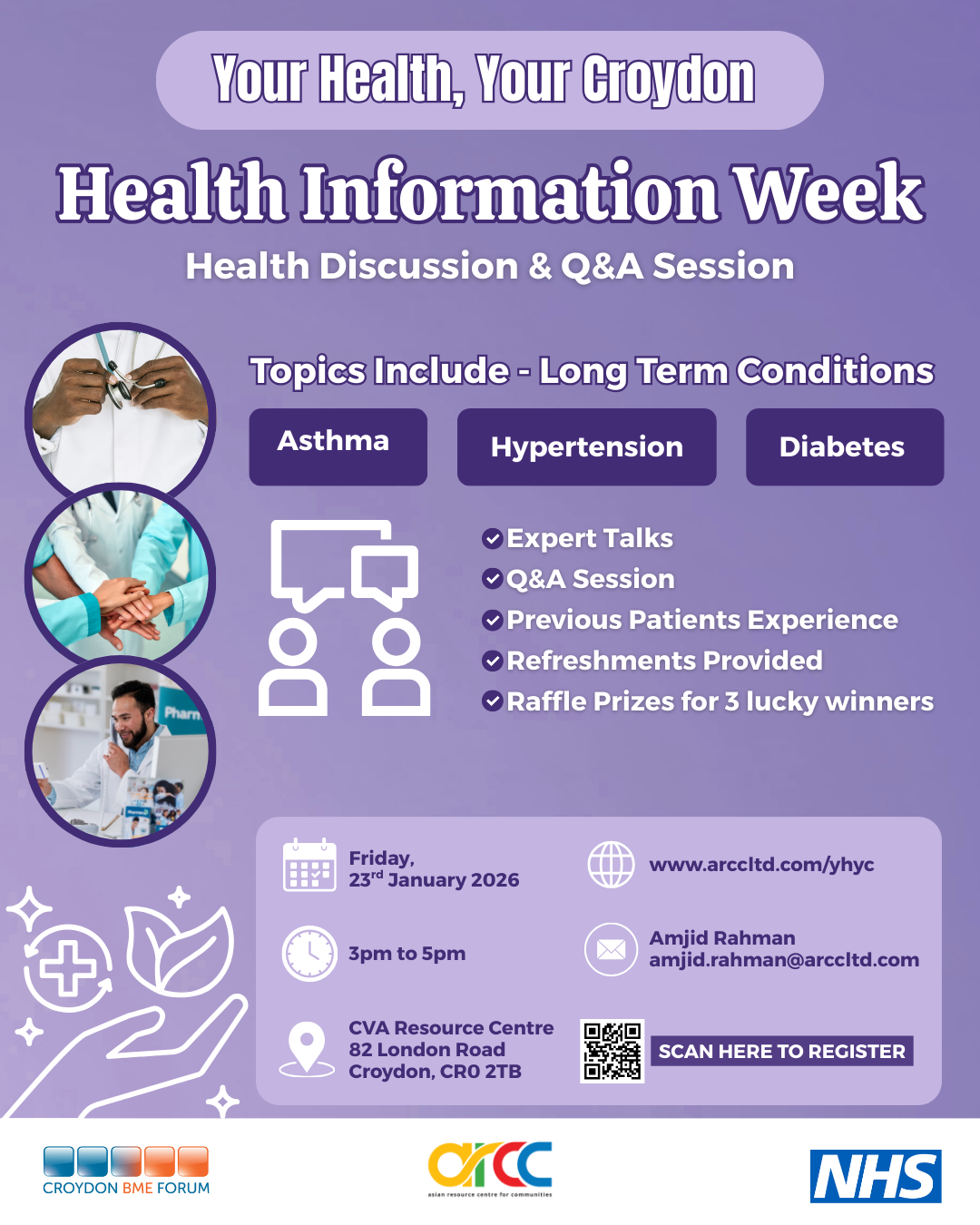
Your Health Your Croydon
Health Information Week